Keratinocytes are instrumental to the epidermal layer of the skin for the barrier formation. Being the primary cells of the epidermis, they are crucial to tissue homeostasis, cutaneous immune response, re-epithelialization, and epidermal repair. The cultivation of human skin epidermal keratinocytes in the in vitro settings enabled extensive research on them, unraveling their role in pathologies such as psoriasis, atopic dermatitis, and melanoma. Researchers have been investigating human skin keratinocytes to develop focused therapeutic modalities.
Brief Role of Human Epidermal Keratinocytes
Keratinocytes are the primary cells of epidermis and constitute 90% of the cells composing the outermost epidermal layer. They perform a range of diverse functions.
- They maintain tissue homeostasis and skin integrity through dynamic signaling pathways.
- When exposed to the external environment, keratinocytes regulate complex immune responses to protect from physical, chemical, and microbial insults.
- They are responsible for vitamin D synthesis and deposition of melanin pigment to shield from UV damage.
- They regulate body temperature and produce sebum and antimicrobial peptides vital to normal tissue function.
Life Cycle of Human Skin Keratinocytes
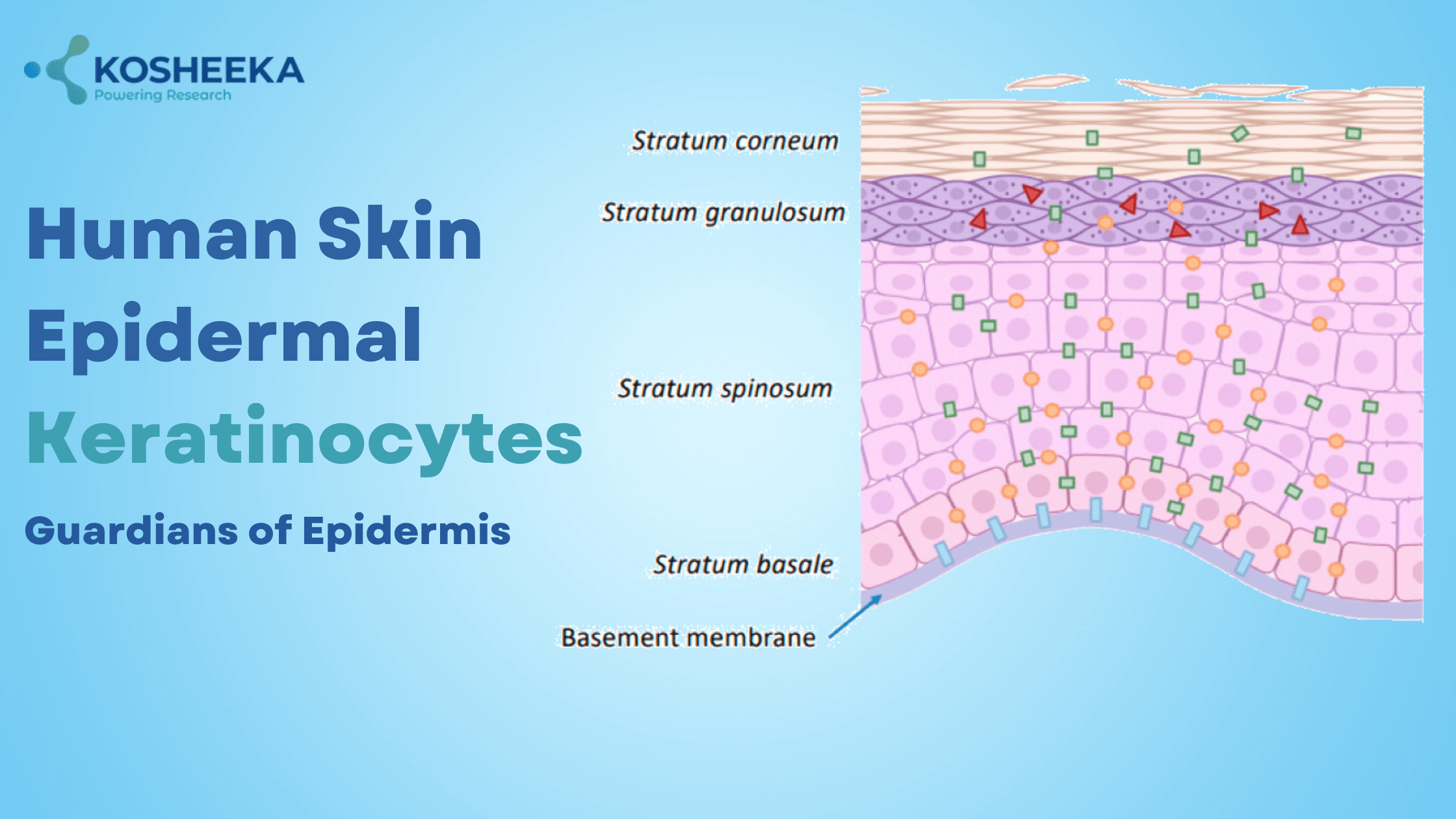
The human skin keratinocytes differentiate to form four different layers ascending from inside to exterior (Fig 1). Epidermis on palms and soles of feet comprises an additional layer beneath the outermost layer named stratum lucidum.
During differentiation, keratinocytes undergo morphological and structural changes along with the production of proteins like keratin, filaggrin, and transglutaminase. Their characteristics vary with their differentiation state, conferring intense complexity to them.
Stratum Basale
This layer comprises the epidermal stem cells that proliferate to form the basal cells. These stem cells divide asymmetrically to produce daughter cells that undergo differentiation in the suprabasal layers. Focal adhesions and hemidesmosomes adhere cells in the basal layer to the basement membrane. Hemidesmosomes use cytoskeletal proteins like keratins for adhesion.
Stratum Spinosum
In this layer, cells lose contact with the basement membrane and shift their keratin filament expression from K5 and K14 to K1 and K10. The adhesion shifts from cell-substrate to cell-cell adhesion via desmosomes. These desmosomes confer a spiny appearance to the layer and maintain the mechanical tension.

Stratum Granulosum
The cells in the granular layer contain lamellar granules that release lipids and proteins (like involucrin and loricrin) in the interstitium of the outermost layer.
Stratum Corneum
In the outermost layer, the plasma membrane of the cells is replaced by an envelope composed of proteins and lipids with 70% loricrin. These cells undergo terminal differentiation, losing their nucleus and assuming a flat shape. This process is referred to as cornification, and the dead cells that pack together to form a physical barrier are termed corneocytes. They use corneodesmosomes for cell-cell interaction. The proteolysis of corneodesmosomes results in desquamation or shedding of corneocytes. Elevated proteolysis is implicated in skin diseases for disrupting the epidermal barrier. Additionally, E-cadherin and gap junctions are also present to maintain the barrier.
Immune Functions by Human Epidermal Keratinocytes
As the outermost layer, skin epidermal keratinocytes are often the first cells to counter pathogens. The pattern recognition receptors (PRRs) in keratinocytes recognize the pathogen-associated molecular patterns like lipopolysaccharides, nucleic acids, endotoxins, lipoteichoic acid, etc. These PRRs include toll-like receptors (TLRs), C-type lectin receptors, and retinoic acid inducible gene I (RIG-I)-like receptors. The ligand binding to PRRs activates the production of inflammatory mediators and antimicrobial molecules.
TLRs: TLR1-6 and TLR9 are upregulated in wounds, which recognize diverse motifs on pathogens. For instance, TLR5 recognizes bacterial flagellin protein, whereas TLR3 recognizes dsRNA from viruses and damaged cells. TLR3 activation further upregulates TLR3 and TLR7 expression, which is not expressed in normal conditions. It leads to a positive feedback loop that results in rapid immune response. TLR3 activation also induces repair and maintenance genes such as TGM1 and ABCA12.
RIG-I-like receptors (RLRs): They are microbial nucleic acid sensors present in keratinocyte cytoplasm and they activate Type I IFN production. The uncontrolled IFN production results in psoriasis. AIM2 is an RLR, which does not trigger IFN production but IL-1β production. IFN-gamma induces AIM2. Strong upregulation of AIM2 causes acute and chronic inflammatory conditions. The stimulator of interferon genes (STING) also participates in this process. Depending on the stimulus, STING can vary the downstream signaling.
Physical Barrier by Human Skin Keratinocytes
Keratinocytes create and maintain a protective barrier. It produces lipids and proteins that combine with the cells in the stratum corneum to form a brick-and-mortar structure. The crosslinked proteins keratin and filaggrin, along with the lipids, line the cornified envelope over keratinocytes, conferring rigidity to the whole layer. Various junctions held the cells tightly together in each layer. The calcium ion concentration gradient regulates these junctions and induces cell differentiation. The continuous cell turnover sustains the low permeability. The cornified cells also maintain slightly acidic pH, limiting pathogen survival while glandular secretions modulate the skin microbiome.
Human Epidermal Keratinocytes in Wound Healing
Wound healing is an intricate multi-step process to restore the epidermal barrier. The last step of the pathway is re-epithelialization. It requires the migration, proliferation, and differentiation of keratinocytes. The re-epithelialization is believed to begin with the dissolution of adhesion molecules, migration of keratinocytes from different layers to the wound, proliferation, and formation of layers of cells. The defects in the migration step often result in chronic wounds.
Mechanotransduction: The process changes the mechanical stress of injury to biochemical pathways. The disrupted junctions and loss of cells during epidermal injury relay mechanical tension to keratinocyte cytoskeleton. The integrin activation at focal adhesion stimulates epidermal growth factor receptor (EGFR) that affects the keratinocyte proliferation.
Migration: Keratinocytes from basal and suprabasal layers develop lamellopodia and migrate to the injury site by weakening cell-cell adhesion. For example, downregulation of E-cadherin, remodeling of hemidesmosomes, and the cytokine-induced synthesis of the keratin filaments K6, K16, and K17 reduce adhesion. Protein kinase C regulates the decrease in desmosome adhesion and the loss of kinase leads to hyper-adhesion by desmosomes and delay in healing.
Immune response: Keratinocytes express receptors for cytokines TNFα and IFNγ. These cytokines induce genes for inflammatory mediators such as IL1 which increases upon skin injury, and IL1β which induces antimicrobial defense. Skin injury increases expression of IL6 receptor on keratinocytes, which induces keratinocyte proliferation by STAT3 signaling. The soluble form of IL6R promotes the barrier repair.
Artificial Skin
The concept of artificial skin emerged with applications in burns, scars, and chronic wounds. The traditional skin graft has limitations like donor skin scarcity and functional impairment of the graft. The cultivation of keratinocytes in the in vitro settings paved the way for artificial skin. It can be acellular, comprising only a matrix, or cellular, consisting of cells on a matrix. Keratinocytes are widely used cells in artificial skin. Artificial skin also has other names like 3D skin, reconstructed skin, skin substitutes, and skin grafts. Several skin grafts, such as EpiDerm (MaTek, USA), EpiSkin (EpiSkin, France), and Apigraf (Organogenesis, USA) are now commercially available.
Product-Related Queries, Or Partnership Inquiries
Pathogenesis of Human Skin Keratinocytes
Disruption in the epidermal barrier leads to several diseases. For instance, filaggrin mutation leads to a dysfunctional barrier, resulting in atopic dermatitis. The skin also sensitizes towards allergens. Mutations in protease inhibitors also cause protease-mediated protein degradation in the barrier, leading to atopic dermatitis. Abnormalities in lipid-producing genes can also disrupt the barrier leading to atopic dermatitis. Disrupted barriers can activate inflammatory response, lowering keratinocyte differentiation and production of antimicrobial agents. On the other hand, psoriasis is a skin inflammatory condition, where excessive antimicrobial peptides react against self DNA.
Conclusion
Keratinocytes are indispensable for structural integrity and tissue functionality. Their differentiation process and immune response sustain a healthy cutaneous barrier protected from external assaults. The disruption of the barrier leads to severe skin diseases. Therefore, researchers are investigating human skin epidermal keratinocytes to detail their role in pathological conditions and develop novel therapies. Kosheeka provides high-quality human skin keratinocytes, ensuring viability, purity, and functionality at low passage to support cutting-edge research in dermatology.
FAQs
Q: What is the role of keratinocytes?
Keratinocytes maintain the skin barrier, defend from pathogen attack by mounting an immune response, and participate in the wound repair process to promote the integrity of the barrier.
Q: What is cornification?
Cornification is the process where keratinocytes undergo terminal differentiation to form the outermost layer of skin.
Several disorders involve keratinocytes and the skin barrier. Atopic dermatitis, melanoma, psoriasis, and lupus erythematosus are a few examples.
Q: What is artificial skin?
Artificial skin is an extracellular matrix composed of polymers. It may or may not contain keratinocytes. It is used as a skin substitute for wound healing.


{kind=link}