
Pancreatic β-islet cells secrete insulin and are critical in the regulation of glucose homeostasis. Their dysfunction causes diabetes mellitus, turning these cells into the focal point of research. Exogenous insulin and insulin-regulating medications have been introduced as the first line of treatment. However, their adverse effects and lifelong dependency have urged the scientists to explore alternative therapies. Consequently, researchers are investigating the signaling pathways, genetic profile, and transcriptional regulation of β-islet cells. They also have applications in drug discovery and screening.
The efficacy and toxicity of the new drugs can be evaluated on these cells. Therefore, understanding the development, structure, and function of Pancreatic β-islet cells is crucial for the formation of effective therapeutic interventions.
Functions of Pancreatic β-islet Cells
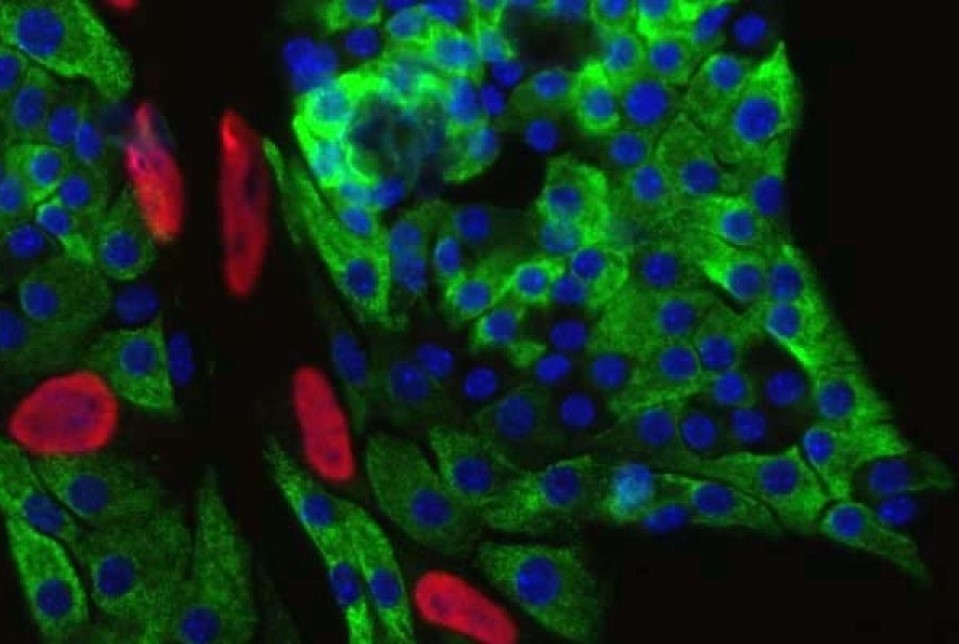
The pancreas acts as an endocrine gland. It comprises cellular aggregates also termed the Islets of Langerhans. They contain four kinds of cells, including β-cells. The functions of β-cells (Figure 1) are:
- synthesize and store the insulin hormone
- sense blood glucose levels
- secrete insulin during high blood glucose levels.
In addition to glucose, these cells also respond to the stimuli from neurotransmitters (norepinephrine, acetylcholine), nutrients (ketones, fatty acids, amino acids), and other hormones (glucagon, gastrin, secretin).
Insulin Secretion Process
Years of research have elucidated the insulin secretion mechanism. The blood glucose enters the cytoplasm of islet cells via glucose transporter (GLUT)- GLUT1 and GLUT2. In the cytosol, glucose undergoes glycolysis followed by the tricarboxylic acid (TCA) cycle and oxidative phosphorylation. The metabolic product, i.e., ATP, is then converted to an electric signal through ATP-based potassium ion channels.
The increase in cytosolic ATP closes these potassium ion channels. It subsequently leads to membrane depolarization, triggering the opening of voltage-dependent calcium ion channels. The resultant calcium ion influx causes the exocytosis of insulin granules.
The hormones trigger β-cells to release insulin granules by stimulating the relevant signaling pathways and activity of ion channels. The nutrients act as metabolic substrates in either glycolysis or the TCA cycle to cause insulin release.
Role of Insulin
Insulin enhances the cellular absorption of blood glucose. Glucose is a vital source of energy. The cellular uptake of glucose involves two types of transporters- sodium ion-dependent and sodium ion-independent. The former absorbs glucose against its gradient by linking to sodium ion transport, whereas the latter transports glucose in accordance with the gradient. The sodium ion-independent transporter, known as GLUT, has seven isoforms. The most common isoforms are GLUT1 and GLUT4. Insulin increases the quantity of these transporters on cell membrane. It leads to augmented absorption of blood glucose and reduced blood glucose levels.
Diabetes Mellitus
Diabetes mellitus is a condition marked with increased blood glucose levels or hyperglycemia. The symptoms include increased thirst, urination, fatigue, etc. However, the persistent high glucose levels in blood can damage vessels and nerves, resulting in visual impairment and limb amputation. The disorder has three broad categories based on its causes.
Type 1 Diabetes Mellitus (T1DM): It is identified as an autoimmune condition where the body’s own immune system destroys β-islet cells. The T1DM individuals have a lifelong dependency on exogenous insulin.
Type 2 Diabetes Mellitus (T2DM): It presents as the development of insulin resistance on body cells. The T2DM patients have functional β-cells that produce insulin. In certain circumstances, high blood glucose can keep triggering insulin synthesis and release, which can lead to β-cell exhaustion and death. It is more prominent in the obese population. A change in lifestyle and diet is recommended in them.
Monogenic Diabetes: It describes the diabetes caused by single gene variations that impair insulin secretion and may also cause insulin resistance. It is further classified into two broad classes- diabetes occurring in infants (known as neonatal diabetes mellitus) and diabetes occurring in young adults due to autosomal dominant inheritance in the family (termed maturity-onset diabetes of the young).
Current Investigative Therapies
The medications for diabetes have severe systemic effects with long-term implications. Therefore, scientists have been attempting different therapies with the aim of increasing insulin secretion and reducing the drug dependency.
Gene Therapy: With the identification of the genes involved in the islet cell development, gene therapy for diabetes became a new avenue for research. It entails the insertion of a therapeutic gene via a vector and its direct administration into the tissue. Gene therapy studies for insulin growth factor 1 (IGF1), glucose 6-phosphatase (G6P), hepatocyte growth factor (HGF), etc. on animal models have resulted in normoglycemia with increased survival and proliferation of β-cells.
Additionally, research also revealed the transcription factors involved in their development and differentiation. The overexpression of these transcription factors (such as neurogenin-3, betacellulin, and pancreas duodenal homeobox-1) by gene therapy also led to normoglycemia, the formation of new islet clusters and transient diabetes reversal.
Cell Therapy
The cell therapy has also shown promise in diabetes treatment. They entail the transplantation of healthy cells to replace dysfunctional or lost cells.
Stem cells: With their differentiation ability, stem cells have found application in the production of healthy β-islet cells. The research has elucidated the signaling mediators that form functional islets from different kinds of stem cells. Additionally, transplantation of mesenchymal stem cells (MSCs) has led to elevated insulin levels by either differentiation into β-cells or stimulating their synthesis.
β-Islet cells: In 2000, Shapiro et al. successfully transplanted islet cells, leading to one year long insulin independence, prompting its use as an alternative therapy. However, it has encountered several challenges on the way, such as limited donor availability, long-term continuation of immunosuppressive regimen, and the limited viability of transplanted cells. The introduction of microencapsulation technology has shown the potential to evade these challenges. Living Cell Technology, an Australia-based organization, has encapsulated pig islet cells and demonstrated positive results in clinical trials. In 2023, the FDA approved an allogeneic islet cell transplantation.
Immune Therapies: These therapies emphasize the prevention of further loss of islet cells instead of regenerating the cells as in other therapeutics. They are particularly beneficial for T1DM patients. The antibodies target the T cells, which are responsible for the autoimmune response. Teplizumab (anti-CD3), anti-thymocyte globulin, alefacept (anti-CD2), and abatacept (anti-cytotoxic T-lymphocyte antigen-4) are few such examples. They have demonstrated improved glycemic control and insulin secretion. There are also antibodies against pro-inflammatory cytokines for treating inflammatory disorders. Their efficacy has also been evaluated for diabetes. These antibodies have protected islet cells against oxidative stress.
Vaccination: The concept of vaccination has emerged to avoid autoimmune response by inducing regulatory T cells and thus, increasing the immune tolerance. Vectors encoding genes for β-islet cell autoantigen or anti-inflammatory cytokines have exhibited increased T cell differentiation towards regulatory T cells in animal models.
Future Trends
While research is progressing in the above-mentioned therapies, new alternatives are emerging simultaneously. In February 2025, a study reported the glucose-dependent release of polymer-coated insulin. The high glucose levels induced a negative potential in the pores of the polymer membrane, which triggered the insulin release. On a similar note, researchers have also created artificial pancreas to sense glucose levels and inject insulin accordingly. However, all these projects are still in the pipeline and might be successful in the future.
Conclusion
A report estimated that approximately 643 million individuals will succumb to diabetes by 2030. Although medications have made diabetes manageable, they have severe cardiotoxic effects. The widespread occurrence of diabetes has prompted the scientists to extensively study pancreatic islet cells to obtain essential insights. They have a vast scope in diabetes research and drug development. Several therapeutic modalities are already under investigation, and the future might witness a definitive cure for diabetes. Kosheeka provides customized human and animal primary pancreatic β-islet cells to enhance your research and accelerate the drug development process. Each batch of these cells are tested negative for HIV, HBV, and HCV. Our team has also evaluated them for viability, functionality, purity, quantity, and sterility. We also fulfill specific donor requirements.
FAQ’s
Q: What is the function of pancreatic β-islet cells?
Pancreatic β-islet cells synthesize insulin, sense blood glucose levels, and release insulin in a glucose-dependent manner.
Q: What are the different types of diabetes mellitus?
There are three broad categories of diabetes mellitus. Type 1 diabetes mellitus loses pancreatic β-islet cells to autoimmune disorder. Type 2 diabetes mellitus shows resistance to insulin, secreted by functional islet cells, by other body cells. Monogenic diabetes has single gene mutations resulting in low insulin secretion.
Q: What are hypoglycemia, hyperglycemia, and normoglycemia?
Hypoglycemia and hyperglycemia denote low and high blood glucose levels compared to the normal glucose range. Normoglycemia describes the glucose levels to be in the normal range.
Q: How does insulin lower blood glucose levels?
Insulin increases the glucose transporters on the cell membrane, thereby increasing the cellular uptake of glucose and lowering the glucose in blood.

{kind=link}